Scalp Psoriasis: Causes, Triggers, Treatment — and What Actually Works in 2026
Scalp Psoriasis:
Causes, Triggers, Treatment —
and What Actually Works in 2026
97% of people with scalp psoriasis say it affects their daily life. The thick silvery plaques. The burning itch that doesn't stop. The treatment that works — until you stop using it. This is the complete clinical picture: what drives it, what triggers it, who gets it, why the standard treatment path has a ceiling, and what a comprehensive approach looks like today.
Scalp psoriasis is an autoimmune condition driven by the IL-23/IL-17 cytokine axis that produces thick silvery-white plaques, intense burning itch, and a relapsing cycle that topical-only treatment cannot break. It affects up to 80% of the 9 million U.S. psoriasis patients. Key triggers include stress, infections, alcohol, and vitamin D deficiency. The 2026 treatment landscape includes roflumilast foam (FDA-approved May 2025), biologics, and plant-based clinical systems designed to support scalp surface renewal, microbiome balance, barrier integrity, and internal nutritional wellbeing — without steroids, coal tar, or a prescription.
- What scalp psoriasis is — and what it looks like
- Prevalence and quality-of-life data
- Symptoms — beyond the flakes
- Triggers — what causes flares
- The IL-23/IL-17 mechanism
- Scalp psoriasis on darker skin tones
- Scalp psoriasis vs dandruff vs seborrheic dermatitis
- Does scalp psoriasis cause hair loss?
- Diet and scalp psoriasis
- The 2026 treatment landscape
- The Dermotricology plant-based protocol
- Frequently asked questions
What Scalp Psoriasis Is — and What It Looks Like
Scalp psoriasis is plaque psoriasis occurring on the scalp. It shares the same underlying autoimmune mechanism as psoriasis elsewhere on the body — the immune system drives skin cells to multiply up to 10 times faster than normal, producing the characteristic buildup of thick, dead skin cells on an inflamed scalp surface. But the scalp presentation is clinically distinct: harder to reach with topical treatments, resistant to standard approaches, and disproportionately impactful on quality of life relative to the area involved.
On lighter skin tones, scalp psoriasis appears as raised, well-defined, reddish or salmon-colored patches covered with thick silvery-white scales. It frequently extends beyond the hairline onto the forehead, back of the neck, and around and behind the ears. On darker skin tones — including Black, Brown, and Hispanic skin — scalp psoriasis may appear purple, violet, or dark brown, with gray rather than silvery scales. This variation is a leading cause of misdiagnosis, discussed in detail below.
A 2025 peer-reviewed network meta-analysis confirmed that scalp psoriasis "is often resistant to topical and conventional systemic agents" and that there is no consensus gold standard treatment.[1] This is the current state of the clinical literature — and the reason a comprehensive multi-driver approach matters.
Prevalence and Quality-of-Life Data
Research presented at the 2025 AAD Annual Meeting confirmed that scalp psoriasis drives severe quality-of-life impact even in patients with low total body surface area involvement.[5] The visibility of the scalp — flakes on every dark shirt, plaques at the hairline — creates a burden that clinical severity scores consistently underestimate. 72.4% of psoriasis patients report activity impairment.[4]
Symptoms — Beyond the Flakes
Scalp psoriasis is frequently reduced to "flaking and itching" in consumer content. The actual symptom profile is significantly more complex — and understanding it matters for both diagnosis and treatment expectations.
- Thick silvery-white plaques — attached to the scalp surface, often with a dry, silvery scale that lifts off and flakes; on darker skin tones these appear gray rather than silver
- Burning itch — not just surface itchiness but deep, persistent burning; the 2025 Sensitive Scalp Syndrome study found 75.1% reported itching as the dominant sensation, followed by prickling, tightness, and burning[3]
- Scalp redness or inflammation — clearly visible on lighter skin; may be subtle or appear as purple/dark discoloration on darker skin
- Extension beyond the hairline — plaques frequently spread onto the forehead, temples, back of the neck, and inside and behind the ears
- Temporary hair thinning — from the chronic inflammation disrupting the follicle cycle (telogen effluvium); typically resolves when the condition is controlled
- Nail changes — pitting, thickening, discoloration, and onycholysis (nail separation) in many psoriasis patients; a key distinguishing feature from seborrheic dermatitis, which does not affect nails
- Sleep disruption — the nocturnal itch from scalp psoriasis is a documented quality-of-life issue affecting sleep and cognitive function
Triggers — What Causes Scalp Psoriasis Flares
Scalp psoriasis is not random. Flares are triggered by identifiable factors that activate or amplify the IL-23/IL-17 inflammatory cascade. Identifying and managing your personal triggers is one of the most effective things you can do to reduce flare frequency — independently of whatever topical treatment you use.
Keeping a simple trigger diary — noting flares alongside stress events, diet changes, weather, sleep, and product changes — is one of the most consistently useful clinical tools for personalizing psoriasis management. The triggers that matter most are specific to the individual, not universal.
The IL-23/IL-17 Mechanism — Why This Is an Autoimmune Condition
Understanding the mechanism isn't just academic — it explains exactly why the relapse cycle exists, why topical-only treatment has a ceiling, and why the most effective pharmaceutical interventions (biologics) work the way they do.
The cascade: from dendritic cells to plaques
Environmental or genetic triggers activate dendritic cells in the skin. These secrete IL-23 — a cytokine that licenses Th17 T-cells to produce IL-17A and IL-22. IL-17A then drives keratinocyte hyperproliferation (skin cells 10× faster than normal), creating the plaque buildup, and generates a feedback loop that sustains the inflammatory environment.[7] This loop doesn't require ongoing external triggering to maintain itself — once established, it is self-perpetuating.
Topical anti-inflammatories suppress the downstream output of this cascade — the visible inflammation and plaque formation — while the upstream immunological loop continues. When you stop, the loop is exactly where it was before. The biologics that produce dramatic results (Skyrizi, Taltz, Cosentyx) work by blocking specific points in the cytokine cascade — which is why their effects are more durable. The access barriers ($25,000+ annually, injections, immunosuppression) leave a real gap that a comprehensive botanical protocol — addressing the internal inflammatory environment alongside the scalp surface — is positioned to fill.
Systemic comorbidities — the same pathway, different tissues
The IL-17 pathway driving scalp plaques also contributes to psoriatic arthritis (up to 30% of patients), cardiovascular disease, metabolic syndrome, and depression through shared inflammatory mechanisms.[7] Severe psoriasis reduces life expectancy by approximately 3–4 years through these comorbidities. This is the clinical rationale for treating psoriasis as a systemic condition — and for including internal support in any comprehensive management protocol.
Scalp Psoriasis on Darker Skin Tones
This section represents one of the most clinically underserved areas in scalp psoriasis content — and given that Kapyderm USA's partner network actively serves patients of all skin tones (including documented clinical outcomes in Black patients with coily hair), it belongs in any comprehensive guide.
On Black, Brown, and Hispanic skin, scalp psoriasis plaques appear purple, violet, or dark brown rather than red, with gray rather than silver scales. Post-inflammatory hyperpigmentation — dark spots remaining after plaques heal — is more pronounced and can persist long after the active disease is controlled. These differences mean it's frequently misdiagnosed as seborrheic dermatitis or "just dandruff."
Black patients are 69% less likely to be prescribed a biologic than white psoriasis patients — a disparity driven by underrepresentation in medical literature, diagnostic undertraining, and insurance access barriers. A plant-based non-pharmaceutical clinical system is particularly relevant for populations who are systematically underserved by the pharmaceutical treatment pathway.[8]
Special considerations for natural and coily hair types
Standard scalp psoriasis treatment advice is designed for straight hair — frequent washing, foam or shampoo-based medicated treatments, leave-on applications. For natural and coily hair types, these protocols don't always translate. Washing frequency may be lower; protective styles (braids, locs, weaves) affect product access; and harsh medicated shampoos may strip moisture from hair types that are already prone to dryness. Botanical oil-based treatments — like K1 Essential Oil and KS115 in the Kapyderm system — offer better compatibility with natural hair care routines than foam or shampoo-only approaches.
Carole Mendoza, Certified Dermotricology Educator at Mendoza Dermotricology Solutions (Pooler, GA), documented a 40-year-old female patient with androgenetic alopecia on tightly coiled natural hair using the Kapyderm plant-based protocol — achieving significant crown density restoration in 16 weeks with zero pharmaceuticals. Read the full case study →
Scalp Psoriasis vs Dandruff vs Seborrheic Dermatitis
These three conditions are among the most confused in scalp health. They share surface symptoms — flaking, scalp discomfort, redness — but have completely different underlying mechanisms, which means they need different interventions.
| Feature | Scalp Psoriasis | Seborrheic Dermatitis | Dandruff |
|---|---|---|---|
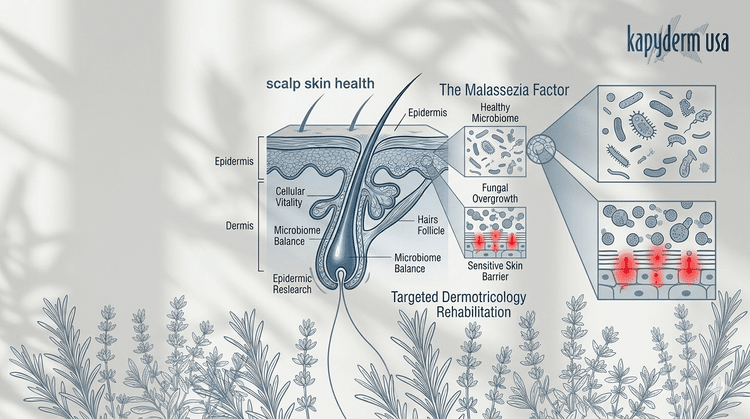
| Mechanism | Autoimmune — IL-23/IL-17 axis | Microbial — Malassezia yeast overgrowth | Malassezia — mild, no significant inflammation |
| Scale appearance | Thick, dry, silvery-white (gray on dark skin); well-defined plaques | Greasy, yellowish, less-defined patches | Loose white or yellowish flakes; fine, not plaque-like |
| Scalp surface | Red/inflamed underneath (purple on dark skin) | Yellowish, oily background | Normal — no significant inflammation |
| Extends beyond hairline | Often — forehead, neck, ears | Rarely | No |
| Burning sensation | Yes — 76.3% have Sensitive Scalp Syndrome | Rarely | No |
| Nail changes | Common — pitting, thickening | No | No |
| Joint symptoms possible | Yes — up to 30% develop psoriatic arthritis | No | No |
| Can overlap | Psoriasis + seborrheic dermatitis together = sebopsoriasis. A 2025 study found SD may be a risk factor for progression to scalp psoriasis. | ||
The critical practical distinction between scalp psoriasis and dandruff: dandruff responds to antifungal shampoos (ketoconazole, zinc pyrithione) because its cause is microbial. Scalp psoriasis does not resolve with antifungal treatment alone because its cause is autoimmune. If antifungal shampoos haven't resolved your scalp condition after consistent use, psoriasis or sebopsoriasis should be considered.
Does Scalp Psoriasis Cause Hair Loss?
Yes — but in the vast majority of cases it is temporary, not permanent. Scalp psoriasis causes telogen effluvium: chronic inflammation disrupts normal follicle cycling, pushing more follicles simultaneously into the resting (telogen) phase, resulting in increased shedding and reduced density. This typically resolves when the condition is controlled — the follicles are dormant, not destroyed.
Permanent scarring alopecia from scalp psoriasis is rare, occurring only in very severe, long-standing, untreated cases where chronic inflammation generates fibrous tissue that permanently replaces the follicle. For most people managing scalp psoriasis, hair loss is a symptom of active disease, not a prognosis for permanent change.
Important note: aggressive scratching, picking at plaques, and certain treatments (high-strength salicylic acid, retinoids) can themselves cause additional hair breakage — independent of the psoriasis itself. Mechanical gentleness with the scalp during active disease is an underemphasized part of hair loss prevention.
Diet and Scalp Psoriasis — The Internal Connection
Diet influences scalp psoriasis through the gut-skin axis and systemic inflammatory load. An anti-inflammatory dietary pattern can reduce the internal environment that sustains the IL-23/IL-17 cascade between flares — making diet one of the most actionable non-pharmaceutical levers in scalp psoriasis management.
- Fatty fish (salmon, mackerel, sardines) — omega-3 fatty acids directly reduce inflammatory cytokine production
- Colorful vegetables and fruits — antioxidants neutralize free radicals that amplify skin inflammation
- Olive oil — oleocanthal has documented anti-inflammatory properties
- Vitamin D — supplementation supports immune regulation; deficiency is a documented trigger
- Probiotic-rich foods (fermented vegetables, kefir, yogurt) — support gut microbiome diversity that modulates systemic immune response
- Whole grains — maintain insulin sensitivity and reduce metabolic inflammation
- Alcohol — dose-dependent trigger; even moderate regular consumption increases flare frequency and reduces treatment effectiveness
- Processed and ultra-processed foods — drive systemic inflammation through advanced glycation end-products
- Refined sugars — spike insulin and amplify the inflammatory cascade
- Red and processed meats — associated with higher systemic inflammatory markers in psoriasis patients
- Nightshade vegetables (tomatoes, peppers, eggplant) — anecdotally reported as triggers by some patients; evidence is individual, not universal
The most evidence-supported dietary pattern for psoriasis is the Mediterranean diet — consistent with the anti-inflammatory priorities above. Emerging research on personalized dietary approaches based on gut microbiome analysis represents the next frontier in dietary management of inflammatory skin conditions.
Obesity and metabolic syndrome are documented psoriasis comorbidities associated with more severe disease and reduced treatment response. Weight management is clinically relevant — not as cosmetic advice but as part of inflammatory load reduction.
The 2026 Treatment Landscape — Honest Assessment
| Treatment | Mechanism | Evidence | Limitations |
|---|---|---|---|
| Coal Tar (T/Gel, MG217) | Slows keratinocyte hyperproliferation; mildly anti-inflammatory | Moderate — NPF-recognized; mild maintenance use | Strong odor; hair discoloration in light hair; potential carcinogenic risk; no microbiome support; no internal component[9] |
| Salicylic Acid (T/Sal, Keralyt) | Keratolytic — softens and lifts scale | Useful for plaque softening; weaker anti-inflammatory | Strips scalp if overused; may cause hair breakage with prolonged use; surface only |
| Clobetasol Shampoo (Clobex) — Rx | Potent corticosteroid — fast suppression of surface inflammation | Strong for moderate-severe; fast clearance | Prescription; HPA axis suppression risk; skin thinning; rebound flare on stopping |
| Roflumilast Foam 0.3% (Zoryve) — Rx May 2025 | PDE-4 inhibitor; steroid-free; once-daily; designed for hair-bearing areas | Strong steroid-free option; well-tolerated; FDA-approved for scalp | Prescription; newer long-term data; topical only; no systemic component |
| Biologics (Skyrizi, Taltz, Cosentyx, Tremfya) | IL-17/IL-23 blockade — targets the systemic driver directly | Excellent for moderate-severe; Skyrizi achieves 83–100% DLQI 0/1 in scalp trials | $25,000+/year; injection or IV; immunosuppression; access barriers for patients of color |
| Oral TYK2 inhibitors (Sotyktu; zasocitinib pending) Emerging | Blocks TYK2 — oral biologic-level efficacy; no injection | Strong phase 3 data; biologic-comparable results without needle | Prescription; black box considerations; newer safety data |
| Kapyderm Scalp Psoriasis Treatment | Intensive keratolytic scale support (KS115) + microbiome rebalancing + barrier support + botanical liver support + nutritional supplementation | Comprehensive plant-based support system for daily scalp management; compatible as adjunct to pharmaceutical care | No steroids · No coal tar · No prescription · 9 components · 2-phase protocol |
The Dermotricology Plant-Based Protocol for Scalp Psoriasis
The Kapyderm approach is designed to address all four scalp drivers simultaneously — intensive keratolytic action to lift surface scale buildup first, then anti-inflammatory botanical support and microbiome rebalancing, then barrier restoration, with internal nutritional support running throughout. The two-phase structure reflects a comprehensive clinical approach: Phase 1 delivers intensive daily support during the active scalp condition; Phase 2 maintains a balanced scalp environment for the long term.
Phase 1 — Intensive Daily Support (during active scalp condition)
Phase 2 — Ongoing Scalp Maintenance
Once the scalp condition has visibly improved and scale buildup has cleared, transition to a daily maintenance routine designed to keep the scalp environment balanced, sebum levels regulated, and the microbiome in a healthy state.
Frequently Asked Questions
- PMC12090945. Biologic and Non-Biologic Therapies for Scalp Psoriasis: Network Meta-analysis of RCTs. Dermatology Practice & Concept. 2025 Apr. PMC12090945
- HCPLive. Psoriasis in 2025: Year in Review. December 2025. 9 million U.S. patients; 80% scalp involvement; roflumilast foam May 2025. hcplive.com
- PMC12721185. Sensitive Scalp Syndrome in Scalp Psoriasis: Prevalence, Correlates, and QoL Impact. JDIN. November 2025. 76.3% SScS prevalence in 350 patients; itching 75.1% dominant. PMC12721185
- PMC3532407. Quality of Life and Work Productivity Impairment among Psoriasis Patients: NPF Survey Data 2003–2011. 88% emotional wellbeing impact; 72.4% activity impairment. PMC3532407
- PhysiciansWeekly / 2025 AAD Annual Meeting. Scalp Psoriasis Drives QOL Impact Despite Low BSA. PSORIATYK SCALP analysis. physiciansweekly.com
- JMIR Dermatology. Google Trends in Dermatology: Scoping Review. Seasonal variation in psoriasis searches — elevated late winter/early spring. derma.jmir.org
- PMC8019008. Interleukin-17 and IL-23: Mechanisms in Psoriasis and Comorbidities. IL-23/IL-17 cascade; 30% psoriatic arthritis; 3–4 yr life expectancy reduction. PMC8019008
- WebMD. How Does Psoriasis Affect People of Color? Black patients 69% less likely to receive biologic prescriptions; misdiagnosis rates; presentation on darker skin. webmd.com
- PMC8163911. Scalp Psoriasis: Literature Review of Effective Therapies and Updated Recommendations. Coal tar compliance issues; carcinogenic risk documented. PMC8163911
- AbbVie / AAD 2026. Risankizumab in Scalp Psoriasis — UnlIMMited Trial. 83.3–100% DLQI 0/1 at 16 weeks. abbvie.com
- Journal of Allergy and Clinical Immunology. Vol. 155, Issue 2. 2025. Multi-omics of seborrheic dermatitis and scalp psoriasis. SD as risk factor for scalp PSO progression; TGM1 and IL36RN as molecular targets. sciencedirect.com
- National Psoriasis Foundation. Scalp Psoriasis. Updated June 30, 2026. Overview, symptoms, causes, triggers, treatment. psoriasis.org
All references are peer-reviewed publications, recognized clinical institutions, or current clinical guidelines. Last reviewed July 2026.
9 Components. Four Scalp Drivers.
No Steroids. No Coal Tar.
The Kapyderm Scalp Psoriasis Home Treatment is a complete plant-based system designed to support scalp surface renewal, microbiome balance, barrier integrity, and internal nutritional wellbeing simultaneously — EU-regulated, compatible with all skin tones and hair types, and formulated for daily use without a prescription.